







A new technology for protecting the cardiac ostium of patients



Surgical team (Dr. Hong Lang, Superintendent of the Hospital, Dr. Wang Hong, Deputy Superintendent of the Hospital, Attending surgeons: Dr. Zeng Hong, Dr. Wang Jing, Dr. Huang Yuan, and Dr. Zhong Kang. Head Nurse Li Jianwen)
A smiling face, a cordial greeting, and a silk banner can be a token of gratitude, recognition, and trust. The cardiac surgical team at Jiangxi Provincial People's Hospital successfully completed a transfemoral-atrial septal access transcatheter mitral valve edge-to-edge repair procedure on an elderly patient on October 29, 2021. The patient made good post-operative recovery and improved their quality of life after the operation. The patient's family specially prepared a silk banner and presented it to Professor Hong Lang and his team as a token of their gratitude, recognition, and trust.
A 69 year-old elderly patient with COPD, type 2 DM, hypertension, and angina was admitted due to sudden onset of chest distress lasting more than 2 weeks. Ultrasonic cardiography revealed posterior mitral valve (P2 region) prolapse with severe concomitant eccentric regurgitation. After repeat evaluation of the patient's general condition and CT findings, Professor Hong Lang and his team of cardiologists reached the consensus that, given the fact that the patient was physically weak and the considerable risks associated with surgery, the patient could not withstand conventional thoracotomy. They decided instead to select a different approach using transcatheter edge-to-edge repair (TEER) via the femoral vein-atrial septum in order to improve the patient's quality of life.

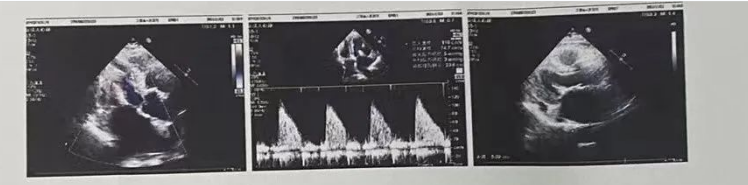
Ultrasonography findings:
2-D and cardiac function: Left atrium I.D. 53 x 56 x 73mm (A-PD x L-RD x I-SD); right atrium I.D. 41 x 62mm (L-RD x I-SD); aortic valve opening of 18mm; aortic annulus I.D. 22mm; ascending aorta I.D. 34mm; aortopulmonary I.D. 21mm; right ventricle outflow tract 20mm; left ventricle end-diastolic diameter 53mm; left ventricle end-systolic diameter 34mm; interventricular septum thickness 10mm, posterior wall thickness of the left ventricle 10mm.
Left ventricular ejection fraction (LVEF): 64%; left ventricular fractional shortening (LVFS): 35%; stroke volume (SV): 86ml; cardiac output (CO): 7.5L.
The left atrium enlarged significantly, the left ventricle was enlarged, the right atrium was enlarged; the rest of the ventricular chamber was normal in size. There was no thickening of the interventricular septum or posterior wall of the left ventricle posterior. Range of motion of ventricular wall acceptable with no notable segment abnormality. The posterior mitral valve was detached towards the left atrium (P2 area and junction of A1 and P1) in the systolic phase, and the chordae tendinae that connects to the posterior valve was ruptured, resulting in poor closure; No morphological and/or structural abnormalities were seen in the rest of the valves. The relation between and development of the large arteries were normal; a liquid dark area was detected in the pericardial cavity; the posterior wall of the left ventricle was approximately 8mm deep, the anterior wall of the right ventricle was approximately 6mm deep, the side wall of the left ventricle was approximately 7mm deep, and the top of the right atrium was approximately 11mm deep.
CDFI: Aortic valve flow velocity Vmax: 1.0 m/s, PG: 4mmHg.
In the systolic phase, massive eccentric regurgitation signals were detected in the left atrium, covering an area of approximately 11cm2: A few regurgitation signals were detected in the right atrium; Vmax: 2.7m/s, PG: 29mmHg, estimated pulmonary artery SBP: 34mmHg.
A few regurgitation signals were detected in the left ventricle outflow tract in the diastolic phase.
Mitral valve diastolic flow E/A<1.
Ultrasound Findings:
Left atrium enlarged significantly, left ventricle enlarged, right atrium enlarged
Posterior mitral valve prolapse (P2 area and junction of A1 and P1) with massive eccentric regurgitation
The chorda tendineae connecting to the posterior mitral valve was ruptured
Minimal tricuspid regurgitation
Minimal tricuspid regurgitation
Left ventricle diastolic function decreased
A small pericardial effusion
During the operation, Professor Hong Lang's team successfully implanted 1 DragonFly valve clip to stabilize the prolapsed valve leaflet; after the implantation, the regurgitation immediately decreased from 3+ to a microamount, and the mean transmitral pressure gradient was 4mmHg, suggesting the patient's hemodynamics were significantly improved and the surgical procedure was highly successful. The elderly patient was discharged on post-operative Day 4 after recovery; when the patient paid a return visit to the hospital for follow-up examination. It was found that the regurgitation was minimal and the patient had no symptoms of discomfort, suggesting good recovery.
Ultrasonography findings:
2-D and cardiac function: Left atrium I.D. 51 x 50 x 67mm (A-PD x L-RD x I-SD); right atrium I.D. 41 x 54mm (L-RD x I-SD); aortic valve opening of 18mm; aortic annulus I.D. 22mm; ascending aorta I.D. 34mm; aortopulmonary I.D. 21mm; right ventricle outflow tract 20mm; left ventricle end-diastolic diameter 46mm; left ventricle end-systolic diameter 30mm; interventricular septum thickness 10mm, left ventricle posterior wall thickness 10mm.
Left ventricular ejection fraction (LVEF): 63%; left ventricular fractional shortening (LVFS): 34%; stroke volume (SV): 61ml; cardiac output (CO): 4.9L.
The bilateral atria was enlarged (mainly the left atrium); the rest of the ventricular chamber was normal in size; there was no thickening of the interventricular septum and/or posterior wall of the left ventricle. The range of motion of the ventricular wall was acceptable; no notable segment abnormality. In the left ventricle short axis view of mitral valve orifice, a valve clip clamping Area 2 of the anterior and posterior valve leaflets and the clamping position remained stable; the mitral valve orifice changed and took on the appearance of a double-orifice; the opening and closing of the valve leaflets were acceptable; No morphological and/or structural abnormality seen in the rest of the valves. The relation between and development of large arteries were normal; a liquid dark area was detected in pericardial cavity; the posterior wall of the left ventricle was approximately 7mm deep, the anterior wall of the right ventricle was approximately 5mm deep, the side wall of the left ventricle was approximately 7mm deep, and the top of the right atrium was approximately 7mm deep.
CDFI: Aortic valve flow velocity Vmax: 1.1 m/s, PG: 5mmHg.
Pulmonary valve flow velocity Vmax: 0.9 m/s, PG: 3mmHg.
The mitral valve forward flow changed and took on a bifurcated appearance, Vmax: 1.2 m/s, PG: 5mmHg, MPG: 3mmHg.
In the systolic phase, regurgitation signals were detected in the left atrium (close to central part of the anterior leaflet); A few regurgitation signals were detected in the right atrium; Vmax: 2.5m/s, PG: 25mmHg; estimated pulmonary artery SBP: 30mmHg.
A few regurgitation signals were detected in the left ventricle outflow tract in the diastolic phase.
Mitral valve diastolic flow E/A<1.
Ultrasound Highlights:
After mitral valve clamping
The position of the mitral valve clip remained stable; no stenosis and only microamounts of regurgitation were detected at the mitral orifice
Bilateral atrial enlargement (obvious in left atrium)
A small amount of aortic and tricuspid regurgitation
Left ventricle diastolic function decreased
A small pericardial effusion
Chief complaints: “tightness of the chest, discomfort, asthenia; diabetes mellitus, and hypertension. When the condition worsened, serious anhelation occurred." The elderly patient said: “earlier I knew that Jiangxi Provincial People's Hospital was a big force in the treatment of cardiovascular disease. I am very lucky to have Professor Hong Lang and his team for the treatment of my disease. I feel relieved and grateful to be treated by them." In the presence of the members of the cardiac surgical team, the elderly patient presented a silk banner printed with the words “Heart-warming medical ethics and consummate medical skills” to Professor Hong Lang to show his gratitude to the professor and the healthcare professionals in the hospital for their painstaking diagnosis and treatment service and premium quality care.
“At Jiangxi Provincial People's Hospital, cardiovascular intervention medicine has made remarkable progress in the independent implementation of multiple new techniques and continual innovation of surgical procedures in Jiangxi Province. The successful application of DragonFly, a Chinese innovative medical device, for transfemoral-transatrial septal transcatheter mitral valve edge-to-edge repair procedure demonstrates the hospital's strength and position in the field of cardiovascular interventional procedures.” Professor Hong Lang commented, “In the future, we will continue to practice mitral valve intervention techniques and provide quality advanced diagnosis and treatment services to more and more patients who suffer from structural heart disease.”
